Pregnancy as a Decision!
The Economic Question of Agency for Women in India?
Nency Agrawal and Samhitha Narayan
Introduction
The latest Nobel prize in Economics awarded to Prof. Claudia Goldin has renewed interests pertaining to women’s role in labour markets. In one of her seminal works, which is broadly referred to as the ‘Quiet Revolution’ article, she argued that there are four phases of women’s involvement in the economy. The first three phases, as she describes to be ‘evolutionary’, largely comprises of three elements, first element being ‘horizon’ of time, or women’s perception regarding the duration of participation in labour market vis-à-vis creation of human capital investment. The second element is ‘identity’ or whether the individuality of a woman is acknowledged in the labour market. The third, in the evolutionary phase is decision making.
This third component of the evolutionary phase is a subtle one and forms the backdrop of this note. In Goldin’s own words: “…whether labour force decisions are made fully jointly, if a woman is married or in a long-term relationship, or, on the other hand, whether the woman is a “secondary worker” who optimizes her time allocation by taking her husband’s labour market decisions as given to her”. Why are we reiterating this? In the contemporary context, marriage and child bearing require further examination in India. This so called ‘prized motherhood’ often limits women to re-enter workforce only after a few years of pregnancy: as the literature would suggest as attrition from the workforce of women. Every year in India, approximately 30 million women go through pregnancy.
It has been noted that the incidence of pregnancy varies significantly across regions and across socioeconomic groups. Beyond India, in the context of the global south the decision of pregnancy and the health outcome literature often emphasises on the role of the public health system (especially roles played by health workers such as ASHA and Anganwadi Workers). These public provisions have improved the health conditions of both the newly born and the pregnant women.
However, there lies a crucial question around the decision of pregnancy. Is it homogeneous across classes, across rural and urban India?

According to research , women from non-Hindu and non-Muslim backgrounds, as well as those belonging to the Other castes (non-scheduled/forward), faced exorbitant maternity care expenses compared to other caste counterparts. Notably, private healthcare facilities are historically associated with mounted financial strains in the Indian context. Household features such as place of residence, women’s education, social group, economic status, and healthcare facility type often influence the qualitative and quantitative differential observed in maternity care expenses in India.
With this in the background, this note aims to bridge a gap: how heterogenous is the incidence of pregnancy across different socio-economic groups? Furthermore, we aim to explore whether there are significant divergences observed in terms of maternity care availed by the households, in terms of costs and choices.
Nomenclature of Pregnancy: 101
Pregnancy care is often subdivided into two parts: prenatal care helps monitor and address potential complications during pregnancy and postnatal care continues this support by monitoring the health of both the mother and child after childbirth. For households in India, expenditure on prenatal and postnatal care represents a significant intra-household economic decision.
Accessible and equitable prenatal care can help prevent complications during pregnancy and childbirth, and can mitigate financial burden associated with vision of prenatal care. Additionally, the utilisation of Postnatal Care (PNC) has been observed to be linked to the education levels of both parents, urban residence, exposure to mass media, and the presence of any pregnancy complications.
While attention in research has been on the impact of public health systems on pregnancy care, few studies have thoroughly investigated the decision of pregnancy. Is there a significant difference across classes with regard to the qualitative nature the decision of bearing a child? Does choice of (or lack of it) healthcare facility and the associated expenditure (therefore the quality of healthcare) during the pregnancy vary differently across caste, class, and location of the household?
Given the substantial divide between rural and urban areas in India, which reflects a profound socioeconomic contrast within the country’s diverse landscape, it is pertinent to analyse pregnancy while focusing on these crucial dimensions.
We have analysed differential outcomes of incidence of pregnancy and costs associated with it that emanates from caste, class, and location of residence (rural/urban) in the contemporary Indian context.
We have used the NSSO 75th Round (2017-18), Expenditure on Social Consumption of Health data to elaborate on these features. In parallel, although NFHS data does provide better information on pregnancy related issues, the last round (NFHS-5) was partly a phone-call survey during the COVID-19 pandemic. This could have jeopardised the quality of the data. Therefore, we have used the NSSO-75th round as the closest alternative to opine on this issue.
Limitations and a Cautionary note on the Database
Before delving into the details, let us outline a few precautions of using NSSO 75th Round data on “Social Consumption in India: Health” data.
To mention, in the previous health-survey round, namely NSSO 71st round (2014), information pertaining to major sources of prenatal and postnatal care did not include records from NGOs and charitable trust hospitals. It did not include informal healthcare providers either. In the NSS 75th round, the survey schedule included these sources among the major providers of prenatal and postnatal care.
Additionally, the NSS 75th round made a distinction between pregnant women as usual members and members from other households who were included solely for childbirth-related purposes, a distinction not made in the NSS 71st round. Therefore, it’s crucial to recognise that these two NSS rounds are not directly comparable.
Furthermore, it is worth noting that the NSS surveys on health has not incorporated government-provided benefits specifically designated for pregnant women during their pregnancies, which is another important consideration in the analysis of maternal healthcare.
A further methodological caveat: we have used the Monthly Per capita Consumption Expenditure (MPCE) quintiles from the household block of the unit level data. These quintiles are used as a proxy for class. We are well aware of the problem with the collection of consumption data in health rounds. The usually expected detailed consumption schedule is not canvassed. Instead, only total monthly consumption expenditure is reported. This might lead to certain incorrect estimations, and could lead to certain problematic benchmarks of class.
However, without any other variable that could refer to income, we stick to the consumption quintiles while acknowledging its limitations. The comparable database of NFHS (National Family Health Survey) was conducted during 2019-21, and due to COVID-induced lockdowns, respondents in some states were surveyed over telephone. Hence, we are using NSSO 75th round for our further analysis.
`
Incidence of Pregnancy: The Myth about Poor in India
The data from the NSSO 75th round in India reveals a noteworthy disparity in pregnancy rates among women aged 15-49, depending on their place of residence. Among women aged between 15-49 years, 6.9 per cent reported being pregnant. In rural areas, this incidence is slightly higher at 7.5 per cent, while in urban areas the reported incidence was roughly 5.4 per cent (See Table 1).
Table 1: Proportion of Pregnant Women Aged Between 15-49 Years, in per cent, by Sector, All India, 2017-18
| Sectors | Proportion of Women Pregnant (%) |
| Rural | 7.5 |
| Urban | 5.4 |
| Overall | 6.9 |
In popular a higher incidence of pregnancy has often been identified as a marker of backwardness. We observe in Table 2, that in both rural and urban areas, the socially marginalised households (SCs and STs) do not have a strikingly higher incidence of pregnancy than the other castes. In rural India, 7.4 and almost 9 per cent women are pregnant from ST and SC households respectively, the incidence is at par with the overall incidence rate of 7.5 per cent for all groups combined (See Table 2).
Although this finding underscores a pattern where rural regions consistently exhibit a higher percentage of pregnant women across various social groups compared to urban areas, when we further break down the numbers across economic locations or class of the households, we observe an interesting puzzle.
This puzzle will perhaps remain as the crux of our note.
In rural areas, more than 60 per cent of pregnant women are in the bottom two or poorest MPCE quintiles, while in urban areas, it is the top two or richest quintiles which contributes to a similar range (See table 2).
Table 2: Distribution of Pregnant Women Aged between 15-49 Years across MPCE Quintiles, By Sector, in per cent, 2017-18
| MPCE Quintiles | Rural | Urban | Total |
| Q1 | 33.2 | 8.3 | 27.1 |
| Q2 | 28.6 | 12.7 | 24.7 |
| Q3 | 21.8 | 16.8 | 20.6 |
| Q4 | 13.1 | 27.6 | 16.6 |
| Q5 | 3.4 | 34.7 | 11.0 |
| Overall | 100.0 | 100.0 | 100.0 |
In urban areas, the top-most quintile (Q5) represents a substantially higher percentage (34.7%) in comparison to the top most quintile (Q5) of rural areas (3.4%). When examining the entire population, it becomes evident that the incidence of pregnancy among rural populace is substantially contributed by the bottom quintiles (Q1 to Q3). Surprisingly, among the urban population the top two quintiles (Q4 and Q5) predominate the incidence of pregnancy reportedly 62.4 % (See Table 2)
This then becomes a myth breaker. The poorer sections or socially marginalised sections in the contemporary Indian context are not the major contributors of the incidence of pregnancy, at least in urban areas.
Is there a regional dimension to this class-wise differences in the incidence of pregnancy? If yes, what causes it? Anecdotally one might argue that rural households with more members are often able to reduce the burden of pregnancy care through the unpaid domestic work provided by other women in the household. For urban India, a strictly higher cost of living and smaller size of the household might make pregnancy a more difficult decision. Even if this explanation was accepted, one observation would remain as a puzzle: with higher public healthcare provisions in India do we still observe burdens (economic and otherwise) that persist in urban India which might reduce the vagaries and costs associate with incidence of pregnancy among poorer women?
We further investigate this concerning puzzle in two ways: First we distinguish between women who receive pre-natal and post-natal care from public agencies vis-à-vis those who receive these services from private agencies. In order to ask, is greater access to and expense on private health care during pregnancy in urban areas increasing the cost of pregnancy care for the masses in overall India?
Paid Cost of Pregnancy: Region Matters!
In prenatal care, as shown in Table 3: urban areas consistently allocate greater resources across all quintiles compared to their rural counterparts.
For instance, within the lowest MPCE quintile (Q1), rural areas expend an average of Rs. 1581 in prenatal care, whereas urban areas demonstrate a more substantially higher expenditure with an average of Rs 2397. In the highest income quintile (Q5), rural areas allocate an average of Rs 4548.5, while urban areas dedicate significantly more, with an average of Rs 6767.2, to prenatal care. On an average, urban areas expend twice as much on prenatal care (Rs 4633.1) as rural areas (Rs 2407.9).
Turning to postnatal care, a similar pattern emerges. Urban areas consistently exhibit higher average expenditures across all MPCE quintiles compared to rural areas. Within the lowest MPCE quintile (Q1), rural areas invest an average of Rs 1044.3 in postnatal care, whereas urban areas allocate more, with an average of Rs 1884.7. In the highest income quintile (Q5), rural areas allocate an average of Rs 2932.7, while urban areas allocate more, with an average of Rs 2941.8 for postnatal care.
Table (3) represents the urban advantage in allocating greater resources for both prenatal and postnatal care across all income quintiles when compared to rural areas. For example, within the lowest income quintile (Q1), rural areas spend an average of Rs 2321.2 on maternal care, while urban areas allocate significantly more, with an average of Rs 3768.5. This pattern remains consistent across all quintiles, with urban areas consistently surpassing rural areas in maternal healthcare expenditure.
Table 3: Average Prenatal and Postnatal and Total Expenditures by MPCE Quintiles, across Sectors, In Nominal Rs., All India, 2017-18
| Prenatal Expenditure | Postnatal Expenditure | Total Expenditure | |||||||
| MPCE Quintiles | Rural | Urban | India | Rural | Urban | India | Rural | Urban | India |
| Q1 | 1581.1 | 2396.8 | 1641.8 | 1044.3 | 1884.7 | 1107.8 | 2321.2 | 3768.5 | 2428.7 |
| Q2 | 2022.1 | 2615.4 | 2096.1 | 1353.8 | 1468.5 | 1368.5 | 2953.2 | 3674.3 | 3042.7 |
| Q3 | 2826.7 | 3330.6 | 2925.5 | 1375.5 | 1855.5 | 1480.9 | 3739.2 | 4759.4 | 3939.2 |
| Q4 | 4004.3 | 4268.4 | 4109.5 | 2155.9 | 1873.8 | 2044.8 | 5565.1 | 5588.2 | 5574.3 |
| Q5 | 4548.5 | 6767.2 | 6253.4 | 2932.7 | 2941.8 | 2939.8 | 6809.9 | 9057.9 | 8536.4 |
| Overall Average | 2407.9 | 4633.1 | 2951.3 | 1423.1 | 2213.8 | 1624.2 | 3398.6 | 6281 | 4100.1 |
When we consider the total average expenditure on maternal healthcare, rural areas report an average of Rs 3,398.6, whereas urban areas nearly double this figure, with an average of Rs 6,281.0. Notably, in Quintile 4, the expenditure on maternal healthcare falls below the overall urban average, while Quintile 5 spends nearly twice that of Quintile 4. This observation raises pertinent questions about whether, in urban India, families’ decisions regarding pregnancy are significantly influenced by their financial capabilities. In essence, the data strongly highlights the urban-rural disparity in maternal healthcare expenditure.
A clear indication of dependence on private health care provision is observed in the upper echelons of the consumption expenditure, especially in Urban India. The top two quintiles in the rural India shows that 30 per cent of fourth quintile and 20 per cent of top quintile receive private health care during pregnancy. While in Urban areas, this is strikingly higher: Almost 56 per cent of top quintile and 37.3 per cent of the fourth quintile take private health care during an ongoing pregnancy (See Figure 2). This perhaps might be indicated further by the costs borne by the households.
Figure 2: Distribution of Women Taking Clinical Treatment During Ongoing Pregnancy, By Type of Clinic and Quintiles of MPCE, in per cent, 2017-18, All India


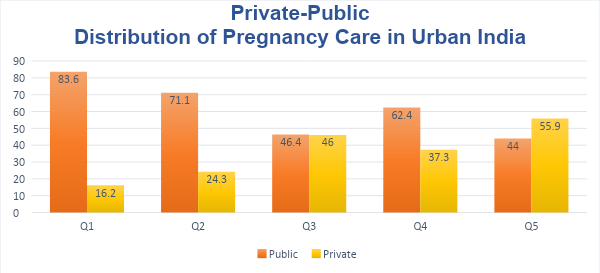


In the context of rural regions, as indicated in Figure 2, it is noteworthy that approximately 74.1% of women opt for public healthcare facilities, while 22.3% choose private healthcare facilities. An interesting pattern emerges when we shift our focus to urban India, where the preference for private healthcare facilities sees a twofold increase, with 41.8% of women favouring them.
Within the lower income quintiles, specifically Quintiles 1 and 2, there isn’t a substantial difference in the choice between public and private healthcare facilities, both in urban and rural areas. However, as we move up the standard of living ladder to the higher income quintiles, particularly in quintiles 4 and 5, a discernible trend emerges. It becomes apparent that women in urban areas display a stronger inclination (55.9%) toward opting for private healthcare facilities, in contrast to their rural counterparts, where only 20.0% choose private healthcare. This shift underscores a significant socioeconomic dimension in healthcare decision-making, where greater financial capacity in urban areas appears to be a driving factor in the preference for private healthcare services.
Women’s Agency or Economic Condition: Revisiting Claudia Goldin
Goldin (2006) emphasised the role that norms and institution going to play with regard to women’s involvement in the economy. This note works as a reminder: involvement is shaped by ‘n’ number of things, often that ‘n’ changes qualitatively.
As an exemplar, we talk about pregnancy in India: where rural regions consistently exhibit higher pregnancy rates but significantly lower maternal healthcare spending and then urban counterparts, highlight that they are (richer ones) affording pregnancy with private care.
Now we ask: Is there a concern that should be reiterated when rural is seen in conjunction with the urban? For private facilities?
Is there an illusory effect expenditure that says: ‘private is better’? Is pregnancy care being is pushed to that and the marginalised sections (in urban India) considering costly health care services as best ones? If pregnancy remains a question of agency of women, this note observes there is no homogeneous decision of pregnancy in India. It’s conditioned by regions, class, and social locations. These differences must make an entry into the policy and academic debates
References/ Endnotes
iGoldin,Claudia (2006): The Quiet Revolution That Transformed Women’s Employment, Education, and Family https://scholar.harvard.edu/files/goldin/files/the_quiet_revolution_that_transformed_womens_employment_education_and_family.pdf
iiIndian Association of Preventive and Social Medicine
iiiHigh Spending on Maternity Care in India: What Are the Factors Explaining It? Srinivas Goli, Moradhvaj, Anu Rammohan, Shruti, Jalandhar Pradhan. Published: June 24, 2016
Authors are Post Graduate students of Economics at the Dr B R Ambedkar School of Economics University, Bengaluru.
Correspondence Email: Nency Agrawal (222pge008@base.ac.in) and Samhitha Narayan (1907PE044@base.ac.in).
Disclaimer: The views and opinions expressed in the blog posts on this website are solely those of the individual authors and do not necessarily reflect the official policy or position of Dr. B. R. Ambedkar School of Economics University. The authors are responsible for the accuracy and completeness of the information presented in their blog posts. The University does not endorse or guarantee the accuracy, completeness, or timeliness of any information provided in these blog posts.